【Axillary Nerve】Pathophysiology and Differential Evaluation Methods of Quadrilateral Space Syndrome (QLSS)
· AcuReco Team · 11 min read
The axillary nerve (C5,6) is an important nerve branching from the brachial plexus, primarily controlling movement and sensation in parts of the shoulder and arm.
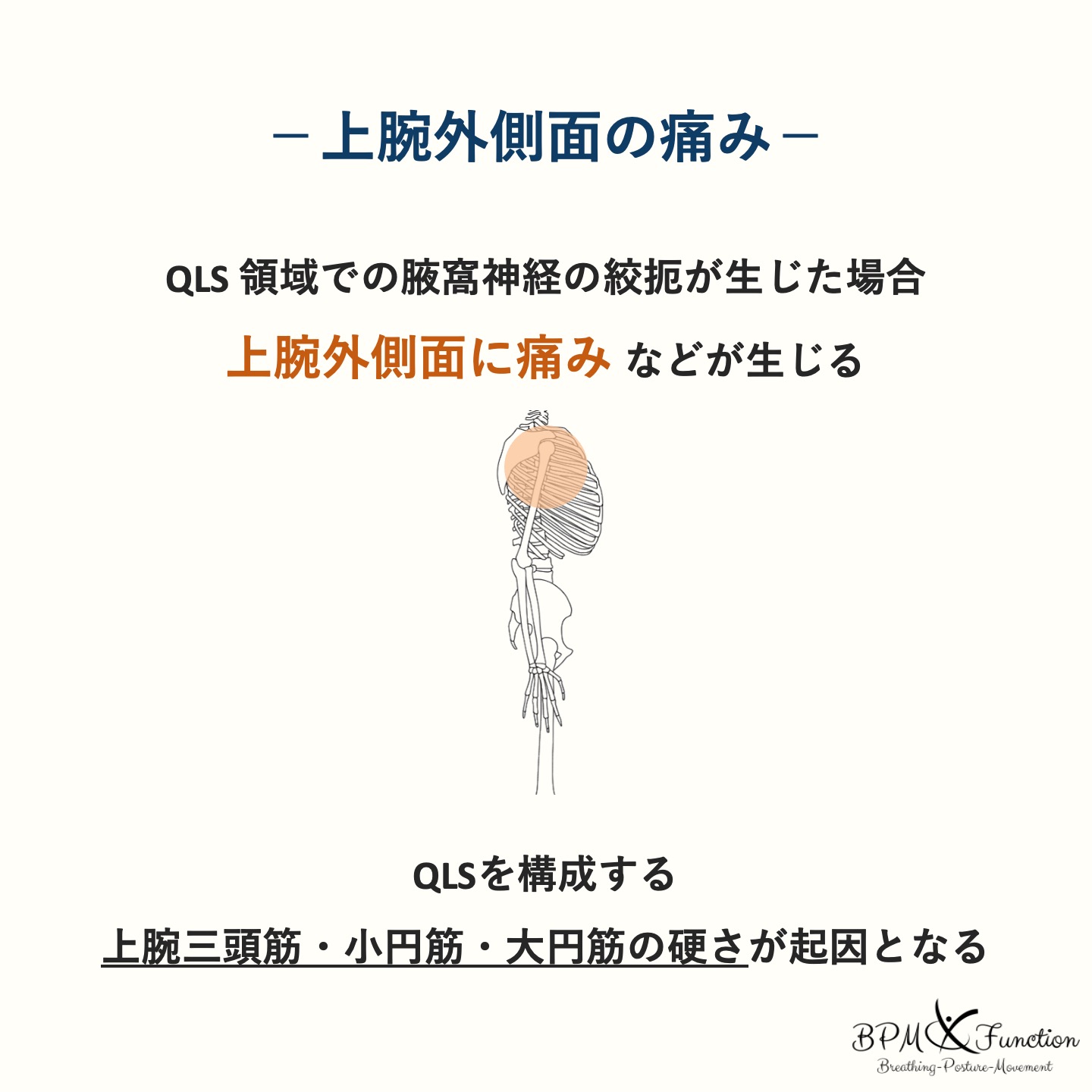
Issues with the axillary nerve can lead to dysfunction of the deltoid and teres minor muscles, making it difficult to raise the upper limb. Sensory problems may include pain or numbness on the shoulder to the lateral side of the upper arm.
In other words, dysfunction of the axillary nerve affects the area around the shoulder joint.

In cases of shoulder joint pain, it is necessary to differentiate between many tissues, one of which is compressive neuropathy of the axillary nerve.
The common site for axillary nerve compression is the "Quadrilateral Space (QLS)".
You may often hear about a condition called Quadrilateral Space Syndrome (QLSS).
This article summarizes the function of the axillary nerve and discusses QLS and QLSS.
Axillary Nerve
The axillary nerve travels as a mixed nerve from the posterior cord of the brachial plexus, passing deeply through the axilla towards the back of the shoulder, under the shoulder joint, and through the Quadrilateral Space (QLS), emerging along the surgical neck of the humerus to the posterior surface of the humeral base.
↓
Deep axilla
↓
From the back of the shoulder under the shoulder joint
↓
Quadrilateral Space (QLS)
↓
Along the surgical neck of the humerus to the posterior surface of the humeral base
Motor Nerve Fibers
The motor nerve fibers of the axillary nerve innervate the deltoid and teres minor muscles.
・Deltoid: Shoulder abduction
Flexion, internal rotation, horizontal adduction (anterior fibers)
Extension, external rotation, horizontal abduction (posterior fibers)・Teres minor: Shoulder adduction, external rotation
Thus, problems with the axillary nerve can make it difficult to raise the upper limb.
Additionally, the teres minor plays an important role in pulling down the humeral head in cooperation with other rotator cuff muscles.
This helps maintain the humeral head in a centered position against the glenoid cavity of the scapula.
For example, dysfunction of the teres minor can lead to issues with the caudal and dorsal glide of the humeral head, potentially causing disruption of the scapulohumeral rhythm and associated shoulder impingement symptoms.
Sensory Nerve Fibers
The sensory terminal branch of the axillary nerve distributes to the skin covering the deltoid muscle.
This branch is called the superior lateral brachial cutaneous nerve.
The superior lateral brachial cutaneous nerve covers the area around the scapular spine on the posterior side and the upper arm and shoulder on the anterior side, providing nerve supply to the entire deltoid muscle.
・Sensory branch of the axillary nerve covering the shoulder to the proximal upper arm
・Distributes to the skin covering the deltoid (especially the upper part)
Summary of the Axillary Nerve
Here is a summary of the axillary nerve as described so far.
・Branches from the posterior cord of the brachial plexus
・Composed of spinal nerves C5,6 at the nerve root level
・Passes from the deep axilla to the back of the shoulder through the quadrilateral space
・Motor nerves innervate the deltoid and teres minor muscles
・Sensory nerves are the superior lateral brachial cutaneous nerve, supplying the shoulder to the lateral side of the upper arm
Isolated paralysis of the axillary nerve can occur due to anterior-inferior shoulder dislocation (or excessive reduction maneuvers), humeral fractures at the surgical neck level, or prolonged axillary pressure from improper use of crutches.
The following section summarizes the understanding of the pathology and differential evaluation methods for axillary nerve compression.
QLS
Quadrilateral Space (QLS) is an important anatomical structure around the shoulder joint, deeply involved in the movement and sensation of the upper limb.
When experiencing shoulder pain, sensory abnormalities, or difficulty moving, it is important to consider this area.
QLS is a quadrilateral space in the axillary and lateral scapular region, formed by the long head of the triceps (medial), humerus (lateral), teres minor (superior), and teres major (inferior).
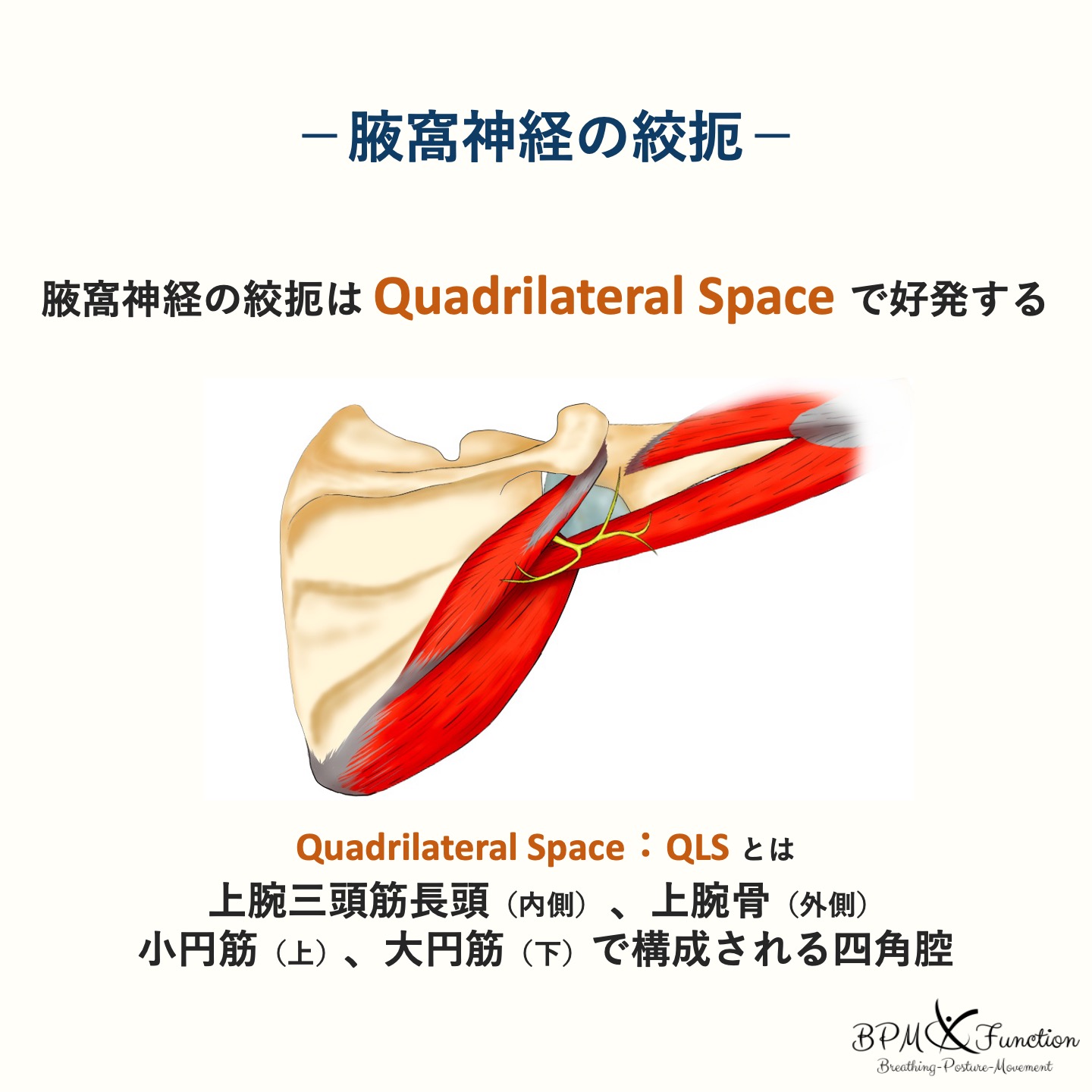
・Long head of the triceps (medial)
・Humerus (lateral)
・Teres minor (superior)
・Teres major (inferior)
Nerves and blood vessels supplying the upper arm pass through here.
The theme of this article, the axillary nerve and the posterior circumflex humeral artery, pass through here, making it essential knowledge for understanding pathology in clinical settings.
・Axillary nerve
・Posterior circumflex humeral artery
The posterior circumflex humeral artery runs alongside the axillary nerve, passing dorsally along the humerus, through the QLS, and along the surgical neck of the humerus to reach the deltoid and shoulder joint. It sometimes anastomoses with the anterior circumflex humeral artery or the profunda brachii artery.
QLSS (QSS)
Quadrilateral Space Syndrome (QLSS) is a condition where the axillary nerve or posterior circumflex humeral artery is chronically compressed in the QLS, causing pain, heaviness, discomfort, or weakness in the shoulder and lateral upper arm.
It is important to understand that it is not only the axillary nerve that is compressed in the QLS, which is crucial for understanding the pathology.
It is better to consider whether the current symptoms are due to compressive neuropathy (neurogenic QSS) or vascular symptoms (vascular QSS), or possibly both.
Also, the fact that symptoms are localized to the shoulder and lateral upper arm is an important point.
Axillary nerve paralysis is a relatively rare symptom, but if shoulder joint dysfunction is prolonged, mild axillary nerve impairment may also be present.
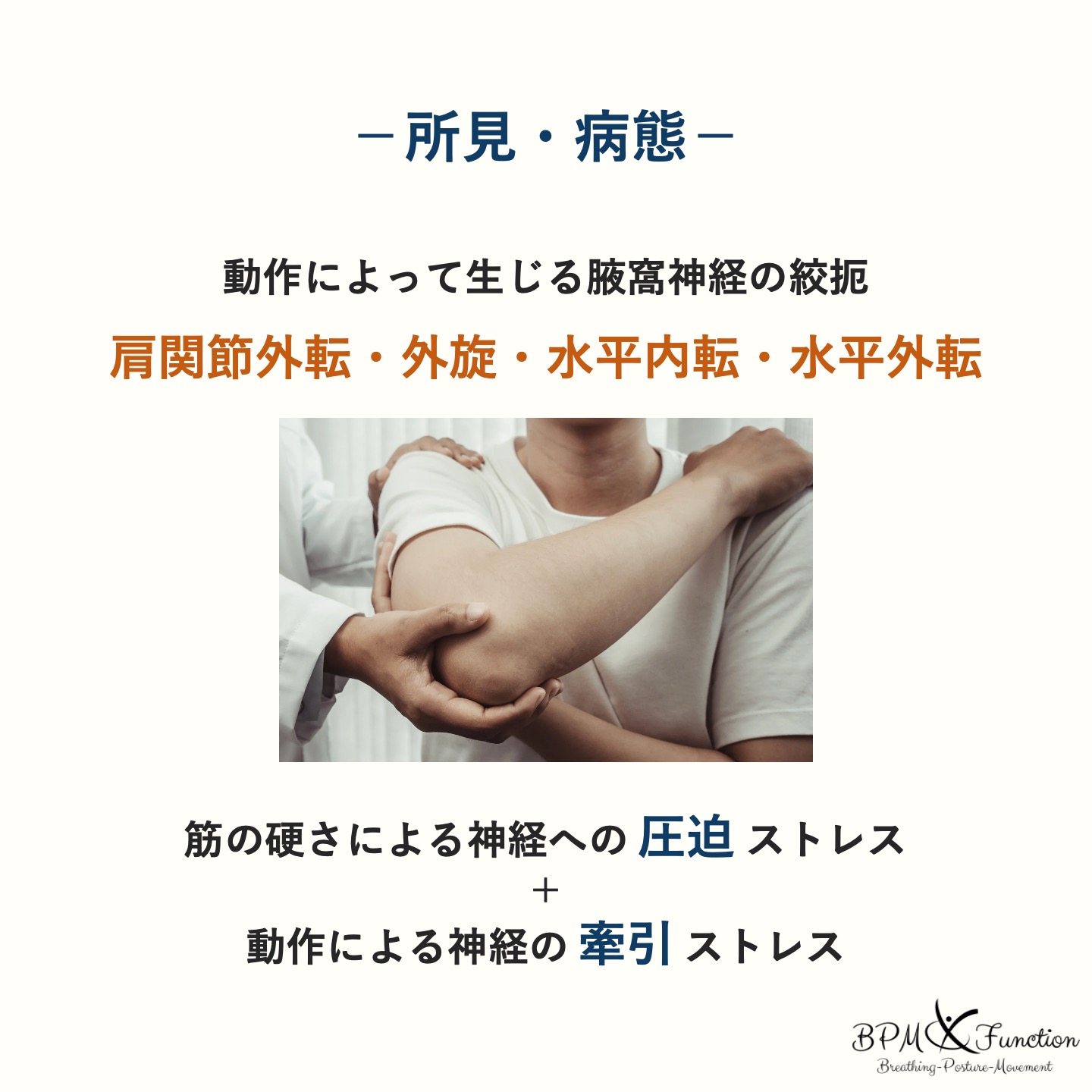
Especially for those involved in overhead sports, increased tension or shortening of the muscles forming the QLS can lead to axillary nerve compression, and the nerve stretching stress from upper limb elevation movements can easily cause symptoms.
In other words, QLSS occurs when compressive stress on the nerve combines with traction stress on the nerve.
Compressive stress on the axillary nerve + nerve stretching stress from movement
Symptoms (Neurological and Vascular)
Symptoms of neurogenic QSS include neuropathic pain, sensory abnormalities, and a sense of weakness.
Symptoms of vascular QSS include ischemic pain or numbness, loss of pulse, and coldness in the hand and fingers.
In addition to these neurological and vascular symptoms, muscle atrophy and the accompanying muscle weakness or debility may occur.
In severe cases, thrombosis of the posterior circumflex humeral artery can block blood flow from the axillary artery, leading to embolism, cyanosis, and ischemia at the distal end of the upper limb, causing coldness.
Differential Evaluation
When performing a differential evaluation of QLSS, it is better to rule out other conditions first, and then conclude that "it might be QLSS!"
This is because QLSS is a relatively rare condition, and patients' complaints are often vague. Additionally, it is necessary to consider imaging findings (MRI or angiography) in collaboration with a physician.
Therefore, diagnosing QLSS can be quite challenging.
Moreover, it is not uncommon for it to coexist with other conditions.
As mentioned earlier, especially in shoulder joint disorders, mild QLSS symptoms may be hidden, so it is advisable to consider them as well.
Understanding the Symptom Location
QLSS is a condition characterized by pain, heaviness, discomfort, or weakness primarily in the shoulder and lateral upper arm.
Therefore, understanding the location of symptoms is crucial for differential evaluation.
Checking Symptom-Inducing Movements
Next, it is important to check the movements that induce symptoms.
Shoulder abduction, external rotation, horizontal adduction, and horizontal abduction may induce symptoms due to compression and stretching of the axillary nerve caused by tension in the muscles forming the QLS.
The following explains the mechanism of symptom induction for each movement.
Shoulder abduction may cause compression on the QLS from the posterior and superior by the teres minor, from the anterior by the teres major, and from the inferior by the long head of the triceps.
Shoulder external rotation, depending on the position, may cause compression on the QLS due to increased tension from shortening of the teres minor and stretching of the teres major.
Shoulder horizontal adduction compresses the QLS from above and below due to stretching of the teres minor and long head of the triceps.
Shoulder horizontal abduction compresses the QLS due to increased tension from shortening of the teres minor and triceps.
Conditions Requiring Differential Diagnosis
The following conditions require differential diagnosis from QLSS.
・Cervical radiculopathy
・Brachial plexus disorder
・Thoracic outlet syndrome
・Subacromial bursitis
・Rotator cuff tear
・Labral tear
・Suprascapular nerve disorder (accessory superior lateral brachial cutaneous nerve)
QLSS symptoms are similar to cervical radiculopathy, brachial plexus disorder, and thoracic outlet syndrome (TOS), so differential evaluation is necessary.
Checking for Tenderness
When symptoms are present on the lateral side of the upper arm, it is very important to check for tenderness in the QLS. If tenderness is present, QLSS should be considered in all cases.
Checking for tenderness in the QLS is simple if you understand the anatomy.
You just need to palpate the intermuscular spaces of the teres minor, teres major, and long head of the triceps...
However, some may find it surprisingly difficult to do it properly.
(By the way, I was not good at it)
For those who struggle, here is a summary of the palpation method for the QLS.
Initially, it is important to palpate carefully. You may become accustomed to it over time and eventually be able to palpate quickly.
Palpation Method
To palpate the QLS, follow these three steps.
① Palpate the axilla with the shoulder joint elevated to 90 degrees
② Repeat external and internal rotation of the shoulder joint to palpate the intermuscular spaces of the teres minor and teres major
③ Repeat elbow joint extension to palpate the lateral side of the long head of the triceps
First, maintain the shoulder joint at about 90 degrees of elevation and palpate the axilla.
At this time, it is best to set the position to whatever allows the patient or client to relax, whether it is below 90 degrees, in flexion, or in abduction.
Then, repeat external and internal rotation of the shoulder joint to palpate the intermuscular spaces of the teres minor and teres major.
Obviously, the muscle that contracts during external rotation is the teres minor, and the muscle that contracts during internal rotation is the teres major.
After palpating these intermuscular spaces, have the patient repeatedly extend the elbow joint to confirm the position of the long head of the triceps.
Once you have identified the position of the long head of the triceps, you should be able to feel a depression just lateral to it. This area is the QLS.
Muscle Differentiation
After confirming tenderness, evaluate which muscle is affected to smoothly transition to treatment and intervention.
First, it is advisable to check for tenderness and palpate muscle tension in the muscles forming the QLS.
Then, check for the presence of muscle shortening.
Considering the function of each muscle, if there is a restriction in internal rotation range of motion in the shoulder flexion position, the teres minor may be shortened; if there is a restriction in external rotation range of motion in the shoulder flexion position, the teres major may be shortened; if there is a restriction in elbow flexion in the shoulder elevation position, the long head of the triceps may be shortened.
However, since joint capsule and ligament extensibility are also involved, it is recommended to consider muscle tenderness and strength as well. If there are findings that can be obtained without spending too much time, it is generally beneficial to collect all of them.
・Checking for muscle tenderness
・Palpating muscle tension
・Evaluating muscle shortening
・Evaluating muscle output
References